The intricate dance of pleasure, often shrouded in mystery, is a universal experience yet varies widely among individuals.
Welcome to our comprehensive exploration of orgasm statistics, where we delve deep into the intimate intricacies of the big ‘O’. From understanding the prevalent ‘orgasm gap’ to uncovering how often women truly climax, our research sheds light on these burning questions and more.
With data-driven insights, we aim to not only inform but also to empower readers with knowledge about this profound aspect of human sexuality.
So, are you ready to unravel the secrets behind one of life’s most exhilarating experiences?
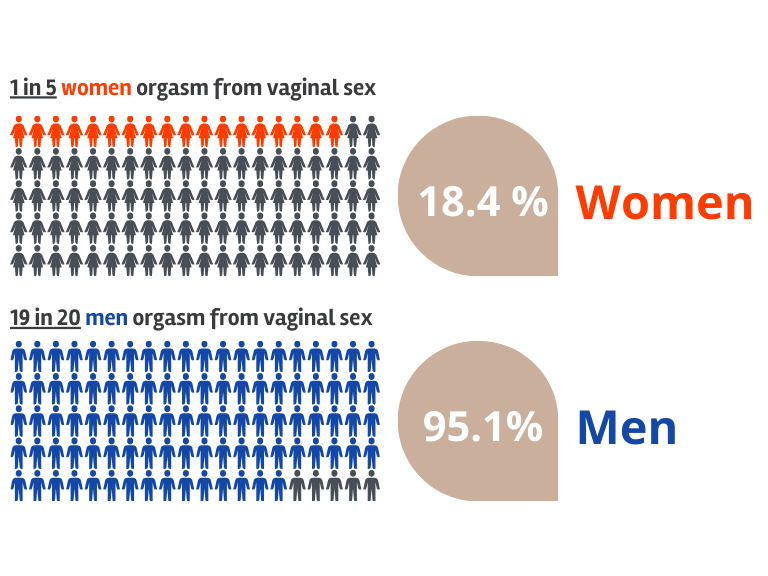
Only 18.4% of women orgasm from penetration/intercourse alone.
92.4% of women are able to orgasm during masturbation.
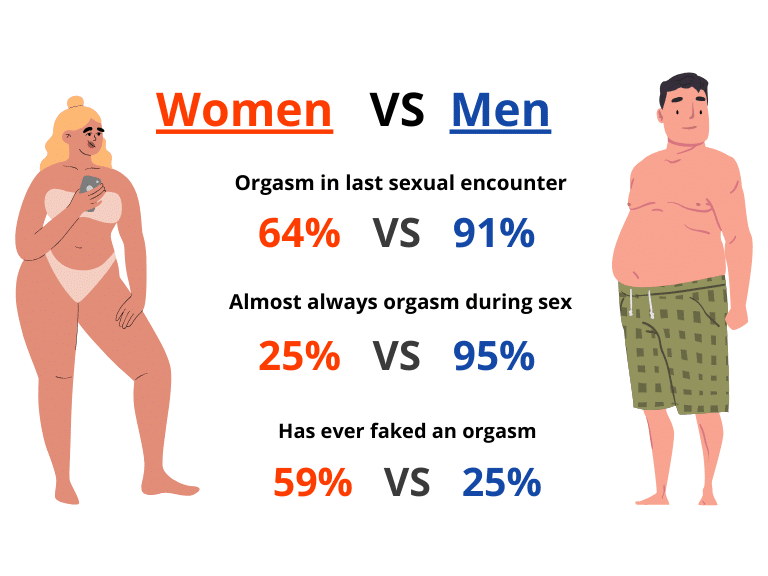
95% of men orgasmed during their last sexual encounter whereas only 65% of women did.
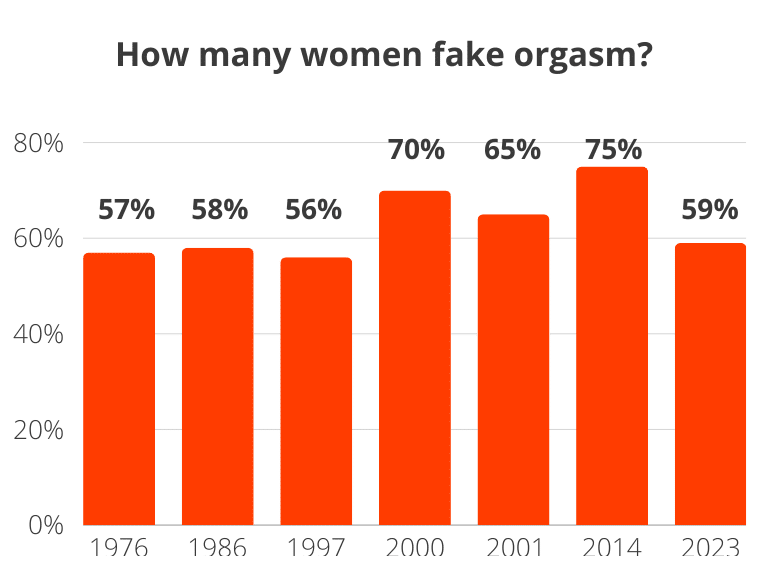
59% of women fake orgasm (only 25% of men do that).
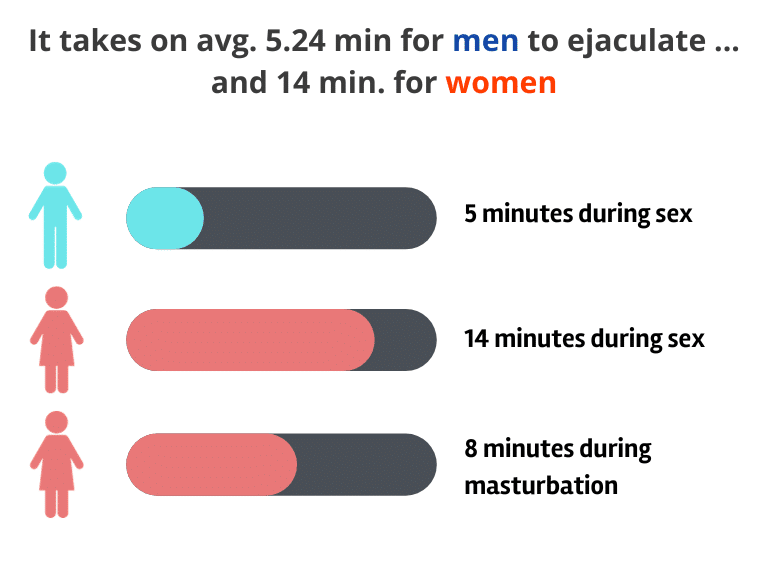
Men on average take 5 minutes to orgasm during partnered sex, while women on average take 14 minutes.
A male orgasm lasts from 6.4 to 56.1 seconds whereas a female orgasm lasts from 17 to 35 seconds.
A male orgasm typically occurs quickly and is stronger, while a female orgasm lasts longer and is weaker.
Women and men should orgasm a minimum of 3 times a week (this relieves stress according to experts).
9 out of 10 women who never had an orgasm manage to reach orgasm after clinical treatment.
11% of women orgasm during their first hookup with a new partner.
Women in relationships for +6 months are 6x more likely to have an orgasm than women who have sex with someone for the first time.
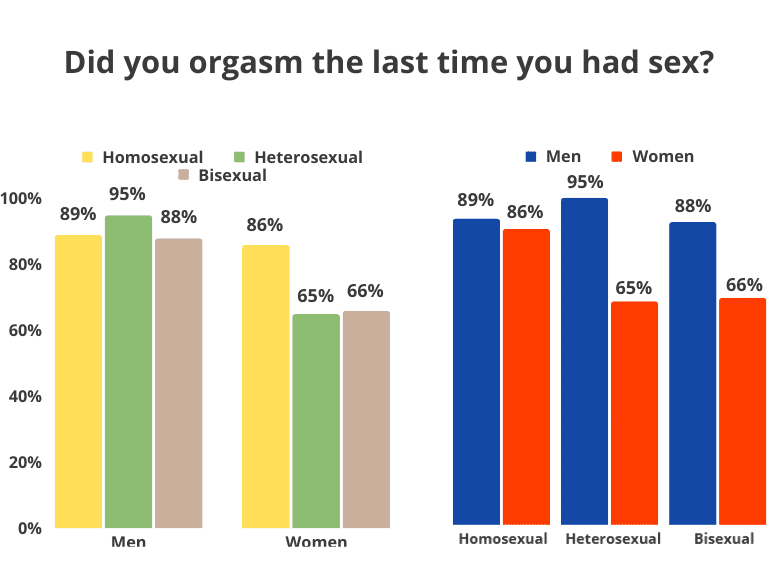
Hetero- and homosexual men are most likely to orgasm. Hetero- and Bisexual women are least likely to orgasm during sex.
The chances of reaching an orgasm go up by 1.6 to 1.8 times when you use your hands to stimulate your partner.
4 out of 10 women have had a sleep orgasm also known as a “wet dream” before age 45.
4 out of 10 men have had a sleep orgasm in their teenage years (13-19 years old).
Orgasm numbers
95.1% of men report that they almost always reach orgasm during intercourse.
18.4% of women say that intercourse without any external stimulation is sufficient for them to orgasm.
64% of women report that they orgasmed in their last sexual encounter.
91% of men report that they orgasmed in their last sexual encounter.
5 out of 10 men think that women reach orgasm 60% of the time.
25% of women report almost always reaching orgasm during intercourse.
51% (to 60%) of women report that they can easily orgasm during vaginal sex if they simultaneously get clitoris stimulation.
The orgasm gap
91% of heterosexual men orgasmed in their last sexual encounter, whereas only 64% of heterosexual women did, making them the least likely.
Men are 280% more likely to report that they almost always orgasm during intercourse compared to women.
Why do we have an orgasm gap between women and men?
The clitoris contains about 8.000 nerve endings. It does feel amazing with intercourse, but the pleasure comes from the clitoris, not the vagina. Most women need direct clitoral stimulation to get an orgasm. So men should focus more on the vagina. Only 18.4% get an orgasm through intercourse.
How many have never had an orgasm?
8.5% of women have never had an orgasm (5-12%, depending on the survey).
92% of women who never had an orgasm before manage to reach orgasm after clinical treatment.
12% of women aged 17-28 years old report that they have never had an orgasm at any point.
30% of women report that they “rarely or never” orgasm during vaginal intercourse.
How does sexual orientation affect orgasm?
During our meta-analysis, we looked at how the data showed differences depending on the sexual orientation of both respondents or study participants.
What we found was quite interesting:
95% of heterosexual men orgasmed during their last sexual encounter.
65% of heterosexual women orgasmed during their last sexual encounter.
89% of homosexual men orgasmed during their last sexual encounter.
86% of homosexual women orgasmed during their last sexual encounter.
88% of bisexual men orgasmed during their last sexual encounter.
66% of bisexual women orgasmed during their last sexual encounter.
By looking into comparing these different groups we find that:
Heterosexual men are 42% more likely to orgasm compared to heterosexual women (95% vs. 65% for heterosexual women).
Homosexual women are almost as likely as homosexual men to orgasm (86% vs. 89% for homosexual men).
Heterosexual females are the least likely group to orgasm compared to men of all sexual orientations as well as compared with both bisexual and homosexual women.
Bisexuality is the sexual orientation amongst men with the lowest chance of reaching orgasm of all other sexual orientations.
Homosexual women are 32% more likely to orgasm compared to heterosexual women (86% vs 65% for heterosexual women, and 66% for bisexual women).
Sexual orientation is a bigger pre-determinant of orgasm frequency amongst women compared to men.
We also look at asexuality, and found that:
Asexuality is not predetermining sexuality for never having reached an orgasm. 77% of asexual women report that they have climaxed before.
How does relationship status affect orgasm?
While looking at the metadata for how different types of relationships and the time they lasted affected the rate of orgasm during intercourse the results were significant. Especially when isolating by gender.
Only 11% of women orgasm during their first hookup with a new partner.
16% of women have experienced an orgasm during the first or second hookup with a new partner.
34% of women report getting orgasms with partners they have had more than 3 hookups with prior.
67% of women in relationships (>6 months) report experiencing orgasms.
Women who have been in a relationship for more than half a year are six more likely to get an orgasm during sex compared to first-time hookups.
Hooking up for the 3rd, 4th, and 5th time improved the odds of reaching an orgasm for women by 40% compared to the first and second hook-ups with a new partner.
Hooking up more than six times makes it twice as likely that the woman will reach orgasm compared to the first hookup.
How do sexual activities affect orgasm?
In the below table, we found the following likelihoods of certain sexual practices to improve the chances of reaching orgasm during sexual intercourse.
Women need to be aroused to get in the “mood”. This will increase the probability for women to orgasm. If women are not aroused before penetration many report that “it hurts a lot!”.
If you stimulate yourself, you are 2.2 to 2.3 times more likely to reach an orgasm during both hookups and in relationships.
If your partner stimulated you, you are 2.3 times more likely during hookups to orgasm (while only 2 times more likely in relationships).
Stimulating your partner with your hands increases the odds of reaching an orgasm by 1.6 to 1.8 times.
Receiving oral sex has a lower chance of getting you to orgasm (1.9 times more likely) compared to if you stimulated yourself with your hands (2.2 times), or if your partner stimulated you with their hands (2.3 times).
Performing oral sex only increases the chance of reaching orgasm if you are in a relationship.
Anal sex does not increase the chance of reaching orgasm in hookups, but it does improve the chance of orgasms by 1.6 times in relationships.
In relationships, receiving oral sex has the biggest effect on the chance of reaching orgasm (by 2.9 times), while it is hand stimulation in hookups that increases the chance of reaching orgasms the most (2.3 times more likely).
Sexual Practices determinant of orgasms
All Hookups
All Relationship Events
Own hand stimulated own genitals
2.19**
2.31**
Partners hand stimulated own genitals
2.25**
1.98**
Own hand stimulated partner genitals
1.62**
1.84**
Received oral sex
1.94**
2.88**
Performed oral sex
1.18
1.20*
Had anal sex
1.43
1.62*
Note: Number represents odds ratios. Meaning that it is X times more likely to result in reaching orgasm. * p < .05; ** p < .01 (two-tailed T-tests).
Masturbation
92.4% of women report that they are able to achieve orgasm during masturbation.
98.7% of men report that they are able to achieve orgasm during masturbation.
82.9% of women report having had their first orgasm through masturbation.
40% of women say they always orgasm when they masturbate compared to 6% during intercourse.
Anal sex
One study reported that all men who reported to have received anal sex achieved orgasm.
The same study indicated that 94% of women orgasmed while receiving anal sex.
Oral sex
Women who receive oral sex are 23% more likely to orgasm during intercourse, compared to men who receive oral sex.
A recent study showed that almost 89% of men have performed oral sex at least once and that 94% of engagers enjoyed it (OrgasmResearchLab).
Right after both women and men orgasm dopamine rushes through the body, click here to read more about what happens the next 60 minutes after an orgasm.
Multiple orgasms
43% of women report that they have experienced multiple orgasms.
2% of women report that they have been able to climax over 20 times during a single session of intercourse/masturbation.
8% of women report having had more than 10 orgasms during a single session of intercourse/masturbation.
Cannabis and orgasms
People report that they on average experience stronger orgasms when using cannabis.
Women on average report having more satisfying orgasms after using cannabis compared to women who did not.
Daily cannabis use in men has been correlated significantly with both reporting of premature ejaculation, and not being able to reach orgasms.
Male prostate orgasms
The frequency of prostate-induced orgasms has a statistically significant positive relationship with lowered risk of prostate cancer in men.
Men who have experienced prostate orgasms report them to be more pleasurable orgasms compared to penile stimulation-induced orgasms.
P. Gałecki, A. Depko, Sylwia Jędrzejewska, M. Talarowska (2012). [Human orgasm from the physiological perspective–part I]. Polski merkuriusz lekarski : organ Polskiego Towarzystwa Lekarskiego
P. Gałecki, A. Depko, Sylwia Jędrzejewska, M. Talarowska (2012). [Human orgasm from the physiological perspective–part II]. Polski merkuriusz lekarski : organ Polskiego Towarzystwa Lekarskiego
Robert Muchembled, J. Birrell (2008). Orgasm and the West: A History of Pleasure from the 16th Century to the Present
5
J. Neuhaus (2000). The importance of being orgasmic: sexuality, gender, and marital sex manuals in the United States, 19220-1963. Journal of the History of Sexuality
A big part of the work we do at Bedbible includes data aggregation, surveying, and studies to help provide our readers with useful insights into a wide range of areas. Including but not limited to sexology, industry research, market size estimations, genders, biases, relationships, and other areas of human interactions.
The team consists of researchers with backgrounds in Political Science, Business intelligence, Cognitive Semiotics, Anthropology, Sexologists, and we frequently work with data scientists and other researchers to gain the deepest data and insight into it. All research insights are published for free on Bedbible.com, and all datasets is released for public access as long as proper accreditation is assigned to any published work using our data.
Feel free to contact us about our backgrounds, analysis, or data sets at: researchcenter@bedbible.com